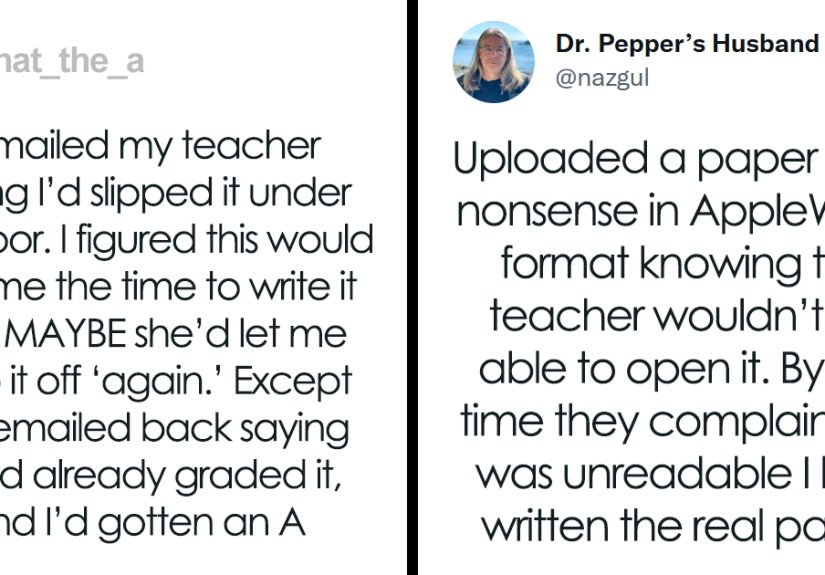



From digital disappearing acts to old-school excuses with shocking confidence, these 30 hilarious homework dodge stories show...
Choosing the best vacuum in 2025 does not have to feel like decoding appliance poetry. This guide...
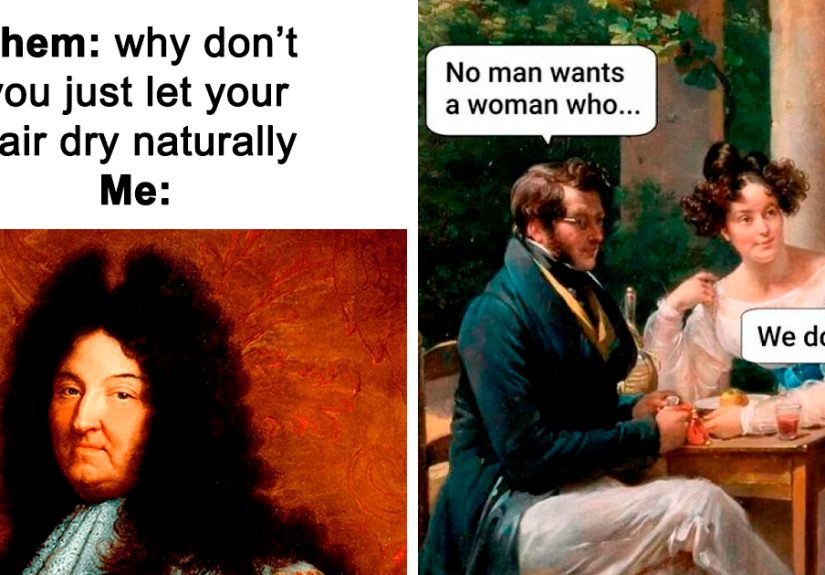
Why do centuries-old paintings feel so accurate in the age of memes? Because dramatic faces, chaotic group...
Is Vaseline a skincare hero or just a greasy old-school classic? This in-depth guide explains the real...

Thinking about a high-velocity HVAC system for an older home or tricky retrofit? This in-depth guide breaks...

Oracle’s acquisition of Cerner was not just a blockbuster deal. It was a high-stakes attempt to repair...
Choosing colors does not have to feel like a guessing game with expensive consequences. This guide breaks...

Keto strawberry shortcakes bring together juicy strawberries, a tender almond flour shortcake, and airy whipped cream in...