




Women physicians navigate career transitions inside a profession that often still rewards constant availability, informal sponsorship, and...
Trying to decide between an internist and a family physician? This in-depth guide breaks down the real...
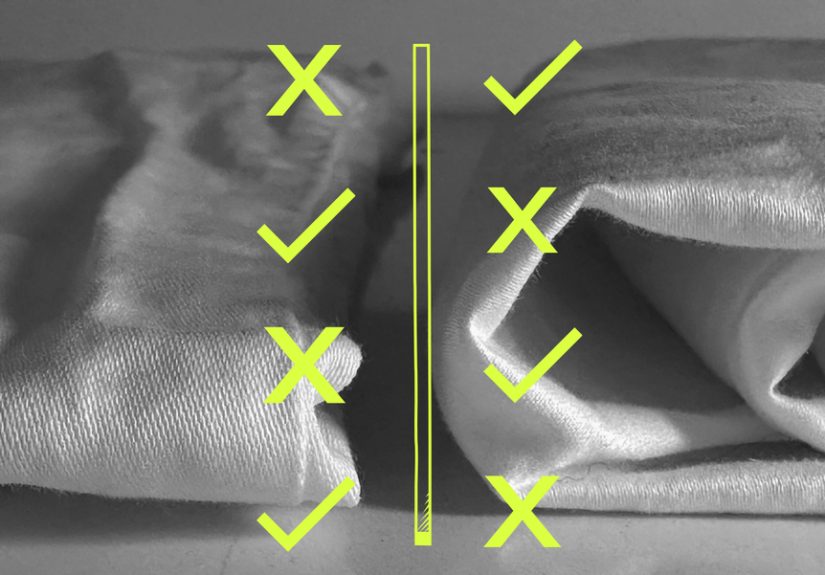
High thread count sheets sound luxurious, but are they actually better? In this in-depth guide, I break...
Messana O’Rorke is a New York architecture and interior design studio known for minimalist spaces that feel...
From crooked tiles and off-center cakes to hilariously bad design fails, these are the 112 photos that...

Recipes and cooking are more than instructions on a page. They are the foundation of better meals,...

Pool coping may look like a simple border, but it does far more than frame your swimming...

Pavan Tavrekere’s striking gallery of colorful spiders and tiny critters proves that the smallest creatures can make...

Want a smarter way to manage ulcerative colitis without drowning in jargon? This Ulcerative Colitis IQ Assessment...

The F-82 Twin Mustang looks like two P-51s fused together, but it’s a purpose-built long-range fighter that...