Table of Contents >> Show >> Hide
- What Is Appendicitis, Exactly?
- Appendicitis Causes
- Appendicitis Risk Factors
- Complications of Appendicitis
- Who Is More Likely to Have Complications?
- Practical Examples of How Appendicitis Shows Up
- How Complications Change Treatment
- Prevention: Can You Actually Prevent Appendicitis?
- Experiences Related to Appendicitis Causes, Complications, and Risk Factors (Extended)
- Conclusion
Appendicitis is one of those medical problems that doesn’t care about your schedule, your plans, or the fact that you
just bought groceries. It’s an inflammation of the appendix (a small, tube-like pouch connected to the large intestine)
that can escalate from “Hmm, my stomach feels weird” to “We should not be at home right now.”
The tricky part? It often starts vague, imitates other issues, and then gets serious if treatment is delayed.
This article breaks down what actually causes appendicitis, who’s more likely to get it, and what complications can happen
if the appendix becomes severely inflamed or perforates. We’ll also cover real-world patterns people noticebecause “it felt
like gas at first” is practically a genre of appendicitis stories.
What Is Appendicitis, Exactly?
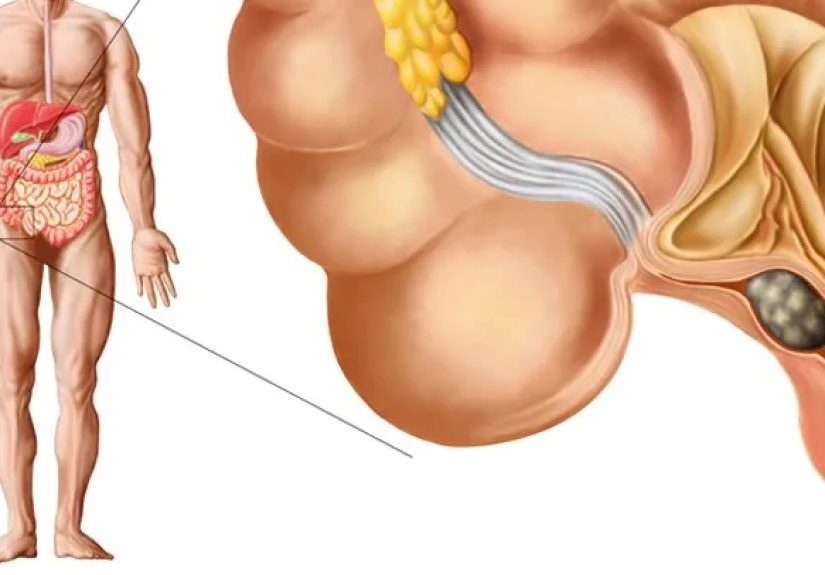
The appendix sits in the lower right side of the abdomen. For a long time, it was treated like a spare part with unclear
purpose, but it’s now considered to have some immune-related functions (especially earlier in life). What matters most in
an appendicitis conversation is this: when the appendix becomes blocked, bacteria can multiply, pressure builds, blood flow
can be compromised, and inflammation ramps up. If the blockage and inflammation aren’t relieved, the appendix can perforate,
spreading infection into the abdomen. That’s why appendicitis is considered a medical emergency.
Appendicitis Causes
Most reputable medical sources describe appendicitis as a problem that usually begins with obstruction (blockage)
of the appendix’s opening or lumen. That blockage sets off a chain reaction: trapped mucus and bacteria increase pressure,
reduce circulation, irritate tissue, and invite more inflammation. (Think: tiny traffic jam, big consequences.)
Importantly, many people never know the exact “single cause”because the obstruction can come from several sources.
Common causes include: (blockage → bacterial overgrowth → inflammation → possible perforation)
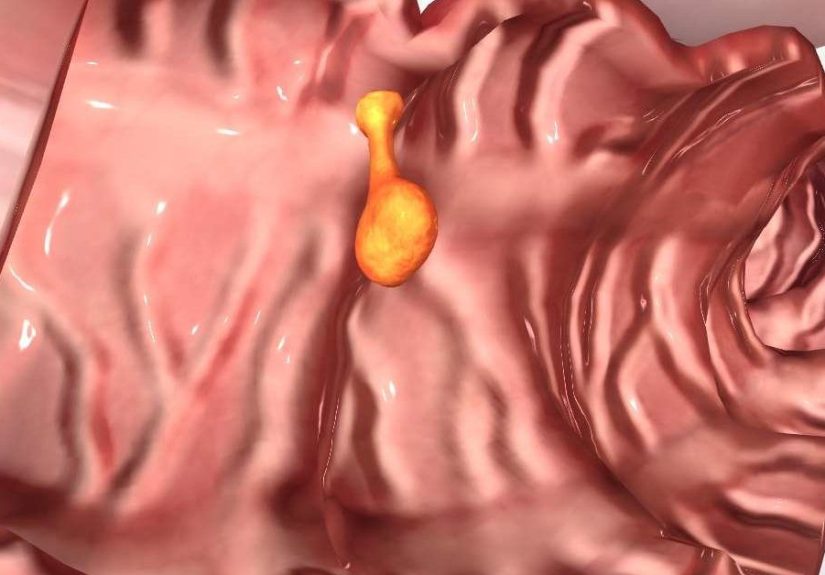
1) Hardened Stool (Fecalith / Appendicolith)
One of the classic culprits is a small piece of hardened stool that blocks the appendix. You’ll see this described as a
fecalith or appendicolith. Once lodged, it can trap material inside the appendix and create the conditions for inflammation
and infection. This mechanism is frequently mentioned as a common cause of acute appendicitis.
2) Swollen Lymphoid Tissue (Often After Infection)
Another common pathwayespecially in children and young adultsis enlargement of lymphoid tissue in the appendix wall.
After viral or bacterial illnesses, lymphoid tissue can swell and narrow the appendix’s opening. Even if the original illness
is “just a cold” or a stomach bug, the swelling can contribute to a blockage in the appendix.
3) Infection and Bacterial Overgrowth
Appendicitis involves bacteria, but it usually isn’t “caught” like a contagious disease. Instead, bacteria that are normally
in the gut can overgrow when the appendix is blocked. The growing bacterial load and rising pressure irritate the appendix,
leading to inflammation.
4) Foreign Body (Rare)
Occasionally, a foreign body can obstruct the appendix. This is uncommon, but it’s part of the broader “something blocked
the opening” category that shows up in clinical references.
5) Tumors (Uncommon, More Relevant With Age)
In a smaller number of casesparticularly in older adultsa tumor in or near the appendix can contribute to obstruction.
This is one reason clinicians take appendicitis in older adults seriously and may consider additional evaluation depending
on the situation.
6) Parasites (Uncommon in the U.S., Mentioned in Medical References)
Some professional references include worms/parasites as a possible cause of obstruction, though this is not a typical explanation
in most U.S. appendicitis cases.
Appendicitis Risk Factors
A “risk factor” doesn’t mean “you will get appendicitis.” It means the odds may be higher compared to someone without that factor.
Appendicitis can still happen to people with no obvious risksbecause the body loves surprises. Still, patterns exist.
Age
Appendicitis is most common in adolescents and young adults, with many sources highlighting teen years through young adulthood
as a peak range. That said, appendicitis can occur at any ageand complications tend to be more common at the extremes (very young
children and older adults) partly due to atypical symptoms or delayed diagnosis.
Sex
Some epidemiologic patterns show appendicitis is slightly more common in males, especially in certain age groups. But from a
practical standpoint, clinicians evaluate symptoms the same way regardless: persistent or worsening abdominal pain needs attention.
Family History and Genetics
Family history appears to increase likelihood. This doesn’t mean appendicitis is “strictly hereditary,” but there may be genetic
or shared environmental factors that influence risk. If multiple close relatives have had appendicitis, it’s worth mentioning to a
clinician when symptoms line up.
Diet Patterns and Constipation
Diet is often discussed in relation to constipation and stool consistency. A diet low in fiber may contribute to harder stools and
constipation in some people, which could theoretically increase the chance of blockage (like a fecalith). The research isn’t as clean
as “eat salad, never get appendicitis,” but fiber-rich eating is generally associated with healthier bowel patterns.
Recent GI Infection
Because swollen lymphoid tissue can contribute to blockage, recent gastrointestinal infections (and sometimes upper respiratory infections)
are sometimes seen in the background story before appendicitis developsespecially in kids and teens.
Inflammatory Bowel Disease and Other Inflammatory Conditions
Conditions that cause chronic inflammation in the digestive tract (like Crohn’s disease) can complicate abdominal symptom evaluation and may
be associated with appendiceal inflammation in some cases. Even when appendicitis isn’t directly caused by IBD, overlapping symptoms can delay
diagnosisraising the risk of complications.
Smoking and Overall Vascular Health
Some observational research suggests smoking may be associated with higher risk of complicated appendicitis (like perforation), possibly through
effects on inflammation and blood flow. This is one of several reasons smoking tends to show up in risk discussions for many acute inflammatory
conditionsnot because it guarantees appendicitis, but because it may worsen outcomes when inflammation hits.
Complications of Appendicitis
Most people treated promptly do well. The danger zone is when inflammation progresses or care is delayedespecially if the appendix becomes
gangrenous or perforates. Complications range from localized pockets of infection to widespread abdominal infection, and they often require more
intensive treatment than uncomplicated appendicitis.
1) Perforation (Rupture)
If pressure and inflammation continue, the appendix can perforate. A perforation allows infected material to escape the appendix. This is a major
turning point because treatment becomes more complex, the risk of infection spreads, and recovery typically takes longer.
2) Peritonitis
Peritonitis is inflammation and infection of the lining of the abdominal cavity. It can occur when a perforated appendix spills infection into the abdomen.
This is serious and requires urgent medical care. It’s one reason clinicians emphasize not “waiting it out” when symptoms are concerning.
3) Abscess (A Pocket of Infection)
Sometimes the body tries to contain the infection by walling it off, forming an abscess. This can happen after perforation, and it may require antibiotics,
drainage, and careful follow-up. Some patients are managed with image-guided drainage and antibiotics depending on clinical stability and imaging findings.
4) Phlegmon (Inflammatory Mass)
A phlegmon is an inflamed, infected mass that can form around the appendix. It’s not a neat “pocket” like an abscessmore like the body’s messy attempt
at containment. Management varies based on severity and imaging.
5) Sepsis (Systemic Infection)
In severe cases, infection can spread beyond the abdomen into the bloodstream, leading to sepsis. This is a medical emergency that can cause widespread
organ stress. While modern treatment has improved outcomes significantly, sepsis remains a key reason appendicitis is treated urgently.
6) Ileus or Bowel Issues During Recovery
Inflammation and infection in the abdomen can temporarily disrupt normal bowel movement, sometimes leading to ileus (a slowdown of intestinal movement).
After surgery, anesthesia and pain medications can also contribute. Most cases resolve with supportive care, but it can prolong hospitalization.
7) Postoperative Infection Risks
Any surgery has infection risks, but complicated appendicitis (especially perforation or abscess) increases the likelihood of postoperative infections,
including intra-abdominal infections. This is why perforated appendicitis is often treated with broader antibiotics and closer monitoring.
Who Is More Likely to Have Complications?
Not all appendicitis cases behave the same way. The risk of complications often rises when diagnosis is delayed or when symptoms are atypical.
Certain groups are more likely to have delayed diagnosis:
Young children
Kids may not be able to describe pain clearly, and symptoms can be nonspecific. Delays can increase perforation risk, which is why persistent abdominal pain,
fever, vomiting, or worsening illness in a child deserves medical evaluation.
Older adults
Older adults may have less “classic” pain patterns and can present later in the disease course. They also may have other health conditions that complicate
assessment, increasing risk of perforation and more serious infection.
Pregnant patients
Pregnancy can shift anatomy and make symptoms harder to interpret. Clinicians often use imaging carefully to evaluate suspected appendicitis, because untreated
appendicitis can be risky for both parent and baby.
Anyone who “toughs it out” too long
The most common human risk factor is hope. Hope that it’s just gas, just stress, just that questionable leftover. Because perforation risk increases with time
in many cases, persistent or worsening symptoms are a reason to get evaluated.
Practical Examples of How Appendicitis Shows Up
Example 1: The “It’s Probably Something I Ate” Start
A teen feels vague belly pain near the belly button, loses appetite, and feels a little nauseated. They try to sleep it off. Over the next several hours, the
pain becomes sharper and settles more on the lower right side. That change in patternalong with worsening discomfort and reduced appetiteis a common
real-world trajectory.
Example 2: The “My Stomach Bug Won’t Quit” Scenario
Someone has vomiting and a low-grade fever and assumes it’s a stomach virus. But the pain persists, localizes, and becomes more severe when walking, coughing,
or moving. When pain becomes more focused and steadily worse, appendicitis moves higher on the list of concerns.
Example 3: The “Older Adult With Weird Symptoms” Situation
An older adult feels generally unwell, with mild abdominal tenderness, fatigue, and reduced appetitewithout dramatic pain. Because symptoms can be less
obvious, evaluation may happen later, increasing the chance of complicated appendicitis.
How Complications Change Treatment
Uncomplicated appendicitis is often treated with appendectomy (surgical removal of the appendix), and in some cases antibiotics may be considered depending on
the clinical scenario. Complicated appendicitis (perforation, abscess, phlegmon, peritonitis) typically involves broader antibiotics and may include drainage
procedures or different surgical timing strategies based on imaging and stability. Clinical pathways used in children’s hospitals, for example, outline different
approaches for non-perforated versus perforated disease.
Prevention: Can You Actually Prevent Appendicitis?
There is no guaranteed way to prevent appendicitis because many cases involve unpredictable obstruction and inflammation. However, general digestive health
habits may help reduce constipation and support gut function:
- Eat a balanced diet with fiber-rich foods (fruits, vegetables, legumes, whole grains).
- Stay hydratedyour colon appreciates the assistance.
- Be physically active, which can support regular bowel movement.
- Avoid smoking for many health reasons, including reduced inflammation and better vascular health.
The most effective “prevention” for serious complications is not lifestyleit’s timing. Early evaluation when symptoms are concerning is what prevents many
complications, especially perforation.
Experiences Related to Appendicitis Causes, Complications, and Risk Factors (Extended)
If you ask people who’ve been through appendicitis what it felt like, you’ll notice a theme: it rarely starts as a neon sign that says “appendix.”
It’s more like a confusing group chat of symptoms where your stomach, your appetite, and your energy all start acting suspicious at once. Many people describe
the first hours as “off” rather than “unbearable.” That’s partly why appendicitis can progressbecause the early stage is easy to minimize.
One common experience is the “maybe it’s constipation” trap. People feel bloated, uncomfortable, and convinced they just need time, water, or a walk.
That’s understandable because one of the classic mechanisms involves blockage, and the sensations can overlap with constipation or gas.
The problem is that appendicitis pain often doesn’t behave like typical indigestion: it tends to persist, intensify, and become more noticeable with movement.
Some people realize something is wrong when standing up, walking, or riding in a car makes the pain sharperlike the body is filing a complaint every time you bounce.
Another frequent story: appetite disappears. Not “I’m not hungry for dessert” but “food suddenly sounds annoying.” This matters because people with appendicitis often
have reduced appetite early. In real life, that might show up as skipping a favorite meal, pushing away snacks, or feeling nauseated at the thought of eating.
Families sometimes notice it before the person doesespecially with kids and teens. A child who normally snacks like it’s a sport, but suddenly won’t eat, gets attention fast.
For teens and young adults (a common age group for appendicitis), there’s also a social reality: they don’t want to “make a big deal.”
Many will try to sleep it off, blame school stress, or assume it’s a random stomach bug. Parents and caregivers often describe a moment when the pain becomes
more localized or the person looks unusually pale and quiet. That’s when “let’s monitor” becomes “we’re going in.” These experiences line up with the idea that appendicitis
can start with vague, central discomfort and then shift as inflammation progresses.
People who end up with complications often describe a timeline problem, not a personality problem. It’s rarely “I ignored it because I’m stubborn” and more often
“I didn’t realize it was serious.” That’s especially true in groups with atypical symptoms:
younger kids who can’t explain pain clearly, older adults who may not get classic pain, or pregnant patients where the body’s changes make everything harder to interpret.
Many families describe a frustrating loop: symptoms seem mild → symptoms fluctuate → symptoms worsen → then suddenly things are clearly not okay.
When perforation or abscess happens, people often report the illness felt bigger overall: higher fever, more fatigue, and a sense that the whole body is involved.
The hospital experience differs depending on whether the appendicitis is uncomplicated or complicated. People with uncomplicated appendicitis frequently describe the
path as surprisingly straightforward: evaluation, imaging, surgery, recovery, home. Many say the hardest part was the uncertainty beforehandwaiting for answers and trying not to Google
themselves into a panic spiral. On the other hand, complicated appendicitis often comes with longer hospital stays, stronger antibiotics, and sometimes drainage procedures or additional monitoring.
Patients may talk about how the care team focused on infection control, hydration, and returning bowel functionbecause once infection spreads beyond the appendix,
the body needs more support to get back on track.
After recovery, a lot of people reflect on risk factors and “what caused it.” Some realize a family member had it at the same age, which makes family history feel less abstract.
Others connect the dots with a recent illness that might have triggered lymphoid swelling. Some never find a satisfying “why,” and that’s normalappendicitis isn’t always a tidy story.
What many people do take away is a practical lesson: persistent, worsening abdominal pain deserves attention, even if it starts vague.
And if you’re in a higher-risk group for complicationsvery young, older, pregnant, or someone whose symptoms are escalatinggetting evaluated early can make the difference between a simple problem
and a complicated one.
The most relatable post-appendicitis comment might be: “I wish I’d gone in sooner.” Not because people love hospitals (they don’t),
but because earlier treatment often prevents perforation, abscess, and prolonged recovery. So if your body is acting like it’s trying to file an urgent report,
it’s okay to listenyour appendix doesn’t hand out medals for endurance.
Conclusion
Appendicitis usually starts with a blockage in the appendix, which can lead to bacterial overgrowth and escalating inflammation. Risk factors such as age (teens and young adults),
male sex, family history, constipation patterns, recent infections, inflammatory conditions, and smoking may influence likelihood or outcomes, but appendicitis can happen to anyone.
The biggest determinant of complications is often time: untreated appendicitis can progress to perforation, abscess, peritonitis, and systemic infection.
If symptoms are persistent, worsening, or don’t fit your usual “stomach bug” pattern, prompt medical evaluation is the safest move.