Table of Contents >> Show >> Hide
- Quick comparison: the “same ingredient, different delivery” story
- What are Concerta and Ritalin, exactly?
- Dosage differences: why milligrams don’t translate 1:1
- How long do they lastand why that changes the “feel”
- Concerta vs. Ritalin LA vs. “regular” Ritalin: don’t mix them up
- Side effects and safety: shared ingredient, shared cautions
- Interactions and “don’t combine” situations
- Which one is “better”?
- Generics and pharmacy substitution: why some people notice differences
- Questions to ask your prescriber (especially when switching)
- FAQ
- Conclusion: the real difference is your day’s rhythm
- Real-world experiences : what people commonly notice with Concerta vs. Ritalin
Concerta and Ritalin are like two coffees made from the same beanssame main ingredient, very different “buzz” schedule.
Both are brand names for methylphenidate, a stimulant medication commonly prescribed for ADHD (and sometimes narcolepsy).
The big difference isn’t what they are; it’s how they release medication in your body, which affects
dosing, timing, and what your day feels like on them.
This guide breaks down dosage forms, typical dosing patterns, and real-world considerations
(school day coverage, appetite, sleep, rebound symptoms, and switching). It’s educationalnot personal medical advice.
For individual dosing and changes, your prescriber should always take the wheel.
Quick comparison: the “same ingredient, different delivery” story
| Feature | Concerta (methylphenidate ER) | Ritalin (methylphenidate IR) |
|---|---|---|
| Release style | Extended-release (once-daily design) | Immediate-release (short-acting) |
| Typical duration | Often described as up to ~12 hours (varies person to person) | Often ~3–4 hours per dose (varies) |
| Typical dosing schedule | Usually once in the morning | Usually 2–3 doses spread across the day |
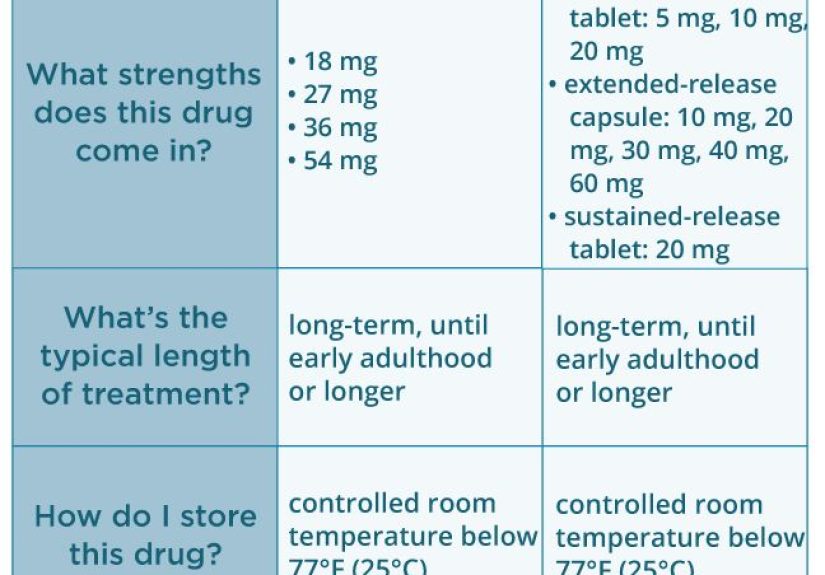
| Strengths (common U.S. brand strengths) | 18, 27, 36, 54 mg tablets | 5, 10, 20 mg tablets (IR) |
| Best for | All-day coverage with fewer “dose reminders” | Flexible timing; shorter coverage; easier fine-tuning |
| Common trade-off | Less flexibility once you’ve taken it | More mid-day dosing and potential “ups and downs” |
What are Concerta and Ritalin, exactly?
Concerta is an extended-release (ER) methylphenidate tablet designed for
once-daily morning dosing.
It uses a long-acting delivery system to spread medication release over many hours.
Ritalin most commonly refers to immediate-release (IR) methylphenidate tablets.
IR forms are typically taken more than once per day to cover a school day, homework time, or work shifts.
(There are also longer-acting methylphenidate products under related brand names, such as Ritalin LA and Ritalin-SR,
which work differently than classic Ritalin IR.)
In plain English: both medications can reduce ADHD symptoms by increasing activity of certain brain chemicals involved in attention and impulse control.
But the release timing changes how steady (or peaky) the effect may feel during the day.
Dosage differences: why milligrams don’t translate 1:1
Here’s the part that causes the most confusion: 18 mg of Concerta is not “the same” as 18 mg of Ritalin IR taken at once.
The number on the bottle is the total methylphenidate in the pill, but the speed of release is different.
Concerta dosing pattern
Concerta is typically taken once daily in the morning.
Because it’s long-acting, prescribers often start low and adjust gradually.
In many clinical references and labeling guidance, children often start at 18 mg once daily, then adjust based on response and tolerability.
Ritalin IR dosing pattern
Ritalin IR is commonly started at a small dose taken twice daily (morning and around lunch),
then adjusted in small steps. Because each dose wears off sooner, it can be easier to “shape coverage”
around specific times of day (for example: mornings are hardest, afternoons are fine).
A practical conversion idea (not a DIY chart)
When clinicians switch someone from methylphenidate IR taken 2–3 times daily to Concerta once daily,
labeling includes conversion guidance. A simplified way to think about it:
Concerta is often used as an all-day substitute for multiple IR dosesbut the exact match depends on your prior schedule,
symptom timing, side effects, and how quickly you metabolize medication.
| Example prior routine (IR methylphenidate total per day) | Example Concerta starting point used in label-based conversions* | What this means day-to-day |
|---|---|---|
| 5 mg taken 2–3 times daily (10–15 mg/day) | 18 mg once daily | Fewer “dose moments,” longer coverage |
| 10 mg taken 2–3 times daily (20–30 mg/day) | 36 mg once daily | Often covers school/work + after-lunch stretch |
| 15 mg taken 2–3 times daily (30–45 mg/day) | 54 mg once daily | Stronger/longer coverage for longer days |
| 20 mg taken 2–3 times daily (40–60 mg/day) | Up to 72 mg once daily (when appropriate and age-eligible) | Maximum-range dosing territory; close monitoring matters |
*Important: This table is a high-level educational summary of common conversion patterns used in official labeling references.
It is not a safe “self-switching” tool. People vary widely in response, and prescribers may choose different steps.
How long do they lastand why that changes the “feel”
Many people describe Concerta as providing longer coverageoften most of the school/work day and sometimes into homework time.
That longer duration can reduce mid-day dosing at school (and reduce the number of times you have to remember medication).
Ritalin IR typically has a shorter window per dose, so you may feel a clearer “start” and “finish.”
For some, that’s helpful: you can target coverage when you need it most.
For others, it can feel like a day of small hills and valleys (focus improves, fades, repeat).
Rebound: the after-effect people don’t always expect
As stimulant effects wear off, some people experience a temporary “rebound”:
irritability, restlessness, emotional sensitivity, or a sudden drop in focus.
This can happen with both medications, but the timing can differ:
IR rebound may show up multiple times per day; ER rebound may show up later in the afternoon or evening.
If rebound is a problem, clinicians often adjust timing, dose, or formulation rather than “power through it.”
Concerta vs. Ritalin LA vs. “regular” Ritalin: don’t mix them up
A lot of online comparisons accidentally compare Concerta to Ritalin LA instead of classic Ritalin IR.
Ritalin LA is a modified-release capsule designed for once-daily morning dosing with a two-phase release.
In some labeling descriptions, certain Ritalin LA capsule strengths are intended to approximate a
“morning + lunchtime” IR schedule.
If you’re trying to compare your prescription to something you read online, check the label:
does it say Ritalin, Ritalin LA, or Ritalin-SR? Those are not identical experiences.
Side effects and safety: shared ingredient, shared cautions
Because both contain methylphenidate, they share many side effects and warnings.
The most common ones people report include:
- Decreased appetite (sometimes leading to weight loss)
- Difficulty falling asleep (especially if taken later in the day)
- Stomachache or nausea
- Headache
- Nervousness or jitteriness
- Increased heart rate or blood pressure (usually small, but monitored)
When side effects are more likely
Side effects often show up most during the first weeks, after a dose increase, or when the timing doesn’t fit the person’s routine.
IR products can sometimes feel “peakier” (a stronger sensation shortly after dosing), while ER products can sometimes feel steadier
but there are plenty of exceptions. Bodies are quirky like that.
Serious warnings to take seriously
Methylphenidate products are controlled substances with a risk of misuse and addiction.
They can also be risky for certain heart conditions and may worsen some psychiatric symptoms in susceptible individuals.
That’s why prescribers screen medical history, monitor growth in children, and check blood pressure and pulse.
Never share your medication, and store it securely.
Interactions and “don’t combine” situations
Some interactions are big enough to be non-negotiable. For example, methylphenidate generally should not be used with
MAO inhibitors (a class of antidepressants) within a certain timeframe, due to the risk of dangerous reactions.
Other medicines and supplements can also interact, including some that affect blood pressure or stimulate the nervous system.
If you’re on any medication for anxiety, depression, blood pressure, seizures, or migrainesor you take “energy” supplements
tell your prescriber and pharmacist. It’s not about getting in trouble; it’s about not accidentally turning your nervous system into a pinball machine.
Which one is “better”?
The most honest answer: neither is universally better.
The better option is the one that matches a person’s schedule, symptom pattern, side effect profile, and access (insurance/pharmacy reality).
Concerta may be a better fit if…
- You want once-daily dosing with longer coverage
- Mid-day dosing at school/work is inconvenient or uncomfortable
- You do better with a steadier effect across the day
- You need coverage into afternoon activities or homework time
Ritalin IR may be a better fit if…
- You want flexibility to target specific times of day
- You prefer a shorter duration (for example, you don’t need evening coverage)
- You and your clinician are fine-tuning dose in small steps
- You’re sensitive to long-acting effects on appetite or sleep
Generics and pharmacy substitution: why some people notice differences
With many medications, “generic” and “brand” feel the same. With some long-acting stimulants, people sometimes notice differences.
One reason: extended-release products depend on delivery technology, not just the ingredient.
The FDA has specifically discussed certain generic versions of Concerta in the past, noting concerns that some products might not provide
the same therapeutic effect for some patients as the brand. The FDA has also described an “authorized generic” that was identical to brand Concerta
under a licensing agreement (availability can change over time).
Practical tip: if you feel a noticeable change after a refillbetter or worsedon’t assume you’re imagining it.
Ask your pharmacist what manufacturer you received, and tell your prescriber what changed (focus coverage, appetite, sleep, mood, rebound timing).
That kind of detail is useful and actionable.
Questions to ask your prescriber (especially when switching)
- What time of day do my symptoms cause the most problems? (Morning classes? Afternoon slump? Evening homework?)
- How will we track effectiveness? (Teacher notes, work output, driving focus, impulsivity, emotional regulation)
- What side effects should I watch for? (Appetite, sleep, mood changes, headaches, stomach issues)
- What’s the plan if it wears off too earlyor too late?
- Are there reasons I should avoid stimulants? (Heart history, certain anxiety patterns, other meds)
If you’re a teen, it’s also reasonable to ask your prescriber how medication fits with school demands, sports, caffeine, and sleep.
(Yes, sleep. The thing everyone tells you to get more of. Annoying, but medically accurate.)
FAQ
Is Concerta just “long-acting Ritalin”?
In a sense, yes: both are methylphenidate. But the delivery system changes how it releases over time, so the experience and dosing schedule can differ.
Can you take them together?
Some clinicians may combine formulations in specific situations (for example, adding a small IR dose at a particular time),
but that decision is individualized and should only be done under medical supervision.
Mixing stimulants on your own is not safe.
What if I miss a dose?
Follow your prescription directions and pharmacist guidance. In general, stimulants taken late in the day can interfere with sleep,
so clinicians often advise against “catch-up dosing” in the eveningbut your prescriber’s instructions are the rule.
Do these medications change your personality?
Ideally, no. The goal is improved attention and impulse control, not turning someone into a different human.
If someone feels emotionally “flat,” unusually anxious, or not like themselves, that’s a reason to talk to the prescriber about dose or formulation.
Conclusion: the real difference is your day’s rhythm
Concerta and Ritalin share the same active ingredient, but their dosage schedules and release profiles can create very different day-to-day experiences.
Concerta is designed for longer coverage with once-daily dosing, while Ritalin IR offers shorter, more flexible coverage that often requires multiple doses.
The right choice depends on when symptoms are most disruptive, how sensitive someone is to peaks and rebound, and what side effects matter most
(appetite and sleep are frequent “deal-breaker” variables).
If you’re considering a switchor trying to understand why two prescriptions with the same ingredient feel differentfocus on timing:
when does it start working, when does it wear off, and what happens in the gap? Those details help a prescriber tailor the plan safely.
Real-world experiences : what people commonly notice with Concerta vs. Ritalin
People’s experiences with ADHD medication are famously variedtwo friends can take the same dose and report totally different days.
Still, there are patterns that show up often in patient and caregiver conversations. Think of the stories below as “common themes,” not guarantees.
1) The “I forgot my lunch dose” school-day problem
A common reason families and teens ask about switching from Ritalin IR to Concerta is simple logistics:
remembering (and being allowed) to take a mid-day dose at school can be a hassle. Some students describe Ritalin IR as
“great in the morning, messy at lunch.” The morning dose helps first and second period, but by midday they feel focus slipping,
and then they’re stuck choosing between visiting the nurse’s office or pushing through until the next dose.
When those students move to a long-acting option like Concerta, the biggest change they notice is not a dramatic personality shift
it’s the relief of fewer medication “events” during the day. Fewer interruptions can feel like smoother momentum:
less time thinking about meds, more time thinking about, you know, the algebra problem that was already rude enough.
2) The “peaks and valleys” vs. “steady cruise control” feeling
Some people describe Ritalin IR as having a clearer on/off switch: focus improves fairly quickly after a dose,
then fades after a few hours. For students, that can be useful when they only need coverage for specific tasks
(tests, tutoring, morning classes). But others experience the day as a roller coaster:
they feel “on” for a while, then “off,” then back “on.” If mood changes or irritability show up when it wears off,
the day can start to feel like a sequence of mini-crashes.
Concerta is often described as more like cruise controlstill with a start and finish, but less dramatic spikes.
People who like it often say it helps them stay more consistently organized: fewer forgotten assignments,
fewer half-started tasks, fewer “I opened my laptop and… somehow ended up reorganizing my entire photo folder.”
People who don’t like it sometimes say the opposite: it lasts too long, or the late-day comedown feels inconvenient.
3) Appetite, timing, and the “dinner comeback”
Appetite changes come up a lot. With IR dosing, some people notice appetite suppression strongest around dose times,
with hunger returning between doses or later in the evening. With Concerta, the appetite effect may feel more “all-day,”
which can be frustrating for anyone trying to eat enoughespecially teens who are growing and active.
A practical theme families mention is the “dinner comeback”: appetite may be low during the day but rebound later,
leading to a bigger dinner or late snack. Clinicians often encourage planning meals intentionally (like eating a solid breakfast)
rather than waiting for hunger signals that may arrive fashionably late.
4) Homework time: the moment of truth
Homework and evening routines are often where differences become obvious. Some students find Ritalin IR works well for school
but wears off before homework. Others find Concerta covers homework betteruntil it doesn’t, or until it interferes with winding down for sleep.
Families sometimes describe a “trade”: better afternoon focus, but more attention to sleep hygiene.
5) The emotional side: focus is not the whole story
People often expect stimulants to only affect attention, but emotional regulation can change toofor better or worse.
Some describe feeling less overwhelmed and more patient because tasks don’t pile up as quickly.
Others feel more tense or irritable, especially if the dose is too high or the medication timing doesn’t match their day.
A repeating theme is that the best outcomes happen when medication is paired with supportive habits:
consistent sleep, predictable routines, therapy or coaching when available, and realistic expectations.
Bottom line: the “best” medication is the one that helps you function and still feels livable.
If the day works but you don’t, that’s not a wintalk to your prescriber about adjusting the plan.