Table of Contents >> Show >> Hide
- What Is a Polypectomy?
- Why Doctors Recommend a Polypectomy
- How to Prepare for a Polypectomy
- What Happens During the Procedure?
- Is a Polypectomy Painful?
- Polypectomy Recovery: What to Expect
- Possible Risks and Complications
- What Happens After the Polyp Is Removed?
- Can Polyps Come Back After a Polypectomy?
- What People Commonly Experience After a Polypectomy
- Final Thoughts
Hearing the word polypectomy can sound like you are about to star in a very serious medical drama, complete with tense music and a surgeon saying, “Scalpel.” In reality, a polypectomy is often much less dramatic. In many cases, it is a minimally invasive procedure done during a colonoscopy to remove a polyp before it causes bigger trouble. That is good news, because many colon and rectal cancers begin as polyps, and removing them early can help prevent cancer from developing at all.
Technically, the term polypectomy can apply to removing polyps from several areas of the body, such as the colon, uterus, nose, or stomach. But when most people search for “polypectomy surgery procedure and recovery,” they are usually talking about a colon polypectomy. This article focuses on that version: what it is, why it is done, how the procedure works, what recovery is usually like, and what happens next once the pathology report comes in.
If you have been told you need a polypectomy, or you already had one and are now Googling every tiny stomach rumble like it is a breaking-news alert, here is what you need to know.
What Is a Polypectomy?
A polypectomy is the removal of a polyp, which is a small growth that forms on the lining of an organ. In the colon, polyps grow on the inner wall of the large intestine or rectum. Many are harmless, but some can become precancerous or cancerous over time. That is why doctors usually remove colon polyps when they find them.
In most cases, doctors remove colon polyps during a colonoscopy or sometimes a flexible sigmoidoscopy. The goal is both diagnostic and preventive. The doctor removes the tissue and sends it to a lab, where a pathologist checks whether the polyp is benign, precancerous, or already cancerous.
One of the biggest misconceptions about polypectomy is that it always means major surgery. It does not. Most polypectomies are endoscopic procedures, meaning the doctor uses tools passed through a scope rather than making a large incision. True surgical removal is usually reserved for polyps that are especially large, hard to reach, suspicious for deeper invasion, or unsafe to remove endoscopically.
Why Doctors Recommend a Polypectomy
Doctors recommend a polypectomy because colon polyps are common, especially in adults over 45, and because some of them can slowly turn into colorectal cancer. A person may have a polyp and feel absolutely nothing. No pain. No warning. No polite memo from the colon. That is one reason screening matters so much.
A polypectomy may be recommended in several situations:
1. A polyp was found during routine screening
This is the most common reason. Colonoscopy is considered the gold standard because it lets the doctor find and remove polyps in the same session.
2. You have symptoms that need evaluation
Sometimes a polyp is found because of rectal bleeding, changes in bowel habits, iron-deficiency anemia, abdominal symptoms, or a positive stool-based screening test. Not every polyp causes symptoms, but when symptoms do show up, they may trigger the workup.
3. You have a personal or family history that raises risk
If you have had polyps before, have inflammatory bowel disease, or have a family history of colorectal polyps or colorectal cancer, your doctor may monitor you more closely and remove any new polyps they find.
4. A large or unusual lesion needs advanced removal
Some polyps are bigger, flatter, or more complex than the usual small bump on a stalk. These may require advanced endoscopic techniques such as endoscopic mucosal resection (EMR) or, in select cases, surgery.
How to Prepare for a Polypectomy
If the polypectomy is being done during a colonoscopy, the preparation is basically colonoscopy prep. And yes, this is the part people complain about with the passion usually reserved for airline delays.
Preparation matters because the cleaner the colon, the easier it is for the doctor to see the lining clearly and remove any polyps safely. If the bowel prep is incomplete, small lesions can be missed, and you may even need another procedure sooner than expected.
Common preparation steps include:
Reviewing your medications: Tell your doctor about prescription drugs, over-the-counter medicines, vitamins, supplements, and especially blood thinners, diabetes medications, or iron.
Changing your diet: You may be asked to avoid high-fiber foods for several days. The day before the procedure often involves a clear-liquid diet.
Drinking the bowel prep: This usually means a laxative solution, sometimes in split doses. It causes diarrhea, so your relationship with the bathroom will become very serious for a while.
Stopping food and drink on schedule: Many patients need to stop eating and drinking by a certain time the night before or the morning of the procedure.
Arranging a ride home: If you receive sedation or anesthesia, you should not drive yourself home afterward.
Follow the prep instructions exactly. This is one of those life moments where “close enough” is not the right strategy.
What Happens During the Procedure?
Most colon polypectomies happen during a colonoscopy in a hospital or outpatient endoscopy center. The procedure itself usually takes somewhere between 15 and 60 minutes, depending on how many polyps are found, where they are located, and how difficult they are to remove.
Step-by-step overview
You receive sedation or anesthesia. Many patients are in a light sleep or deep sedation and do not remember much of the procedure. For smaller lower-colon procedures such as flexible sigmoidoscopy, sedation may not always be needed.
The doctor inserts the colonoscope. A thin, flexible tube with a light and camera is gently passed through the rectum and into the colon. Air or carbon dioxide is used to expand the colon for a better view.
The doctor inspects the colon lining. As the scope advances and is slowly withdrawn, the doctor looks for polyps, abnormal tissue, bleeding, or other changes.
The polyp is removed. The exact technique depends on the size and shape of the polyp:
Forceps removal
Very small polyps may be removed with tiny biopsy forceps.
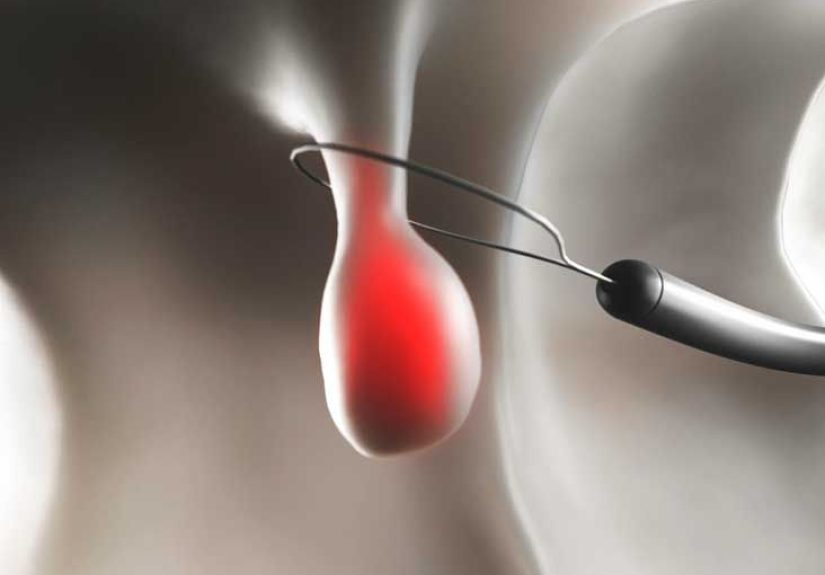
Snare polypectomy
Small to medium polyps are often removed with a wire loop called a snare. The loop fits around the base of the polyp and cuts it off. Sometimes electrical current is used to cut the polyp and reduce bleeding.
Cold snare vs. hot snare
A cold snare polypectomy removes the tissue without heat and is commonly used for smaller polyps. A hot snare polypectomy uses electrocautery and may be used for some larger lesions.
Endoscopic mucosal resection (EMR)
Larger flat polyps may require EMR. In this technique, fluid is injected underneath the lesion to lift it away from deeper layers, creating a safer cushion for removal. EMR can often remove lesions that once required traditional surgery.
Endoscopic submucosal dissection (ESD) or surgery
Some very large or complex lesions need advanced endoscopic resection, staged removal, or referral to a specialist. If a lesion cannot be removed safely through the scope, surgery may be recommended.
Once removed, the tissue goes to pathology. That lab report becomes a major part of your follow-up plan.
Is a Polypectomy Painful?
During a colonoscopy-based polypectomy, most people do not feel the actual removal. What you may feel is cramping, pressure, bloating, or gas from the air used during the exam. If you are sedated, you may remember very little. Many patients say the procedure itself was easier than the prep, which is a bit like saying the roller coaster was fine but the line was terrible.
Afterward, mild soreness, cramping, bloating, and fatigue are common. If a large lesion was removed, you may need more recovery time and more detailed aftercare instructions.
Polypectomy Recovery: What to Expect
Recovery after a routine polypectomy is usually quick. Most patients go home the same day. If sedation was used, you will spend some time in recovery while it wears off. The rest of the day is usually for resting, hydrating, and taking it easy.
The first few hours
You may feel sleepy, groggy, gassy, or mildly crampy. Bloating is common because air was used during the procedure. Walking can help move the gas along. Light bleeding from the rectum may happen, especially if a polyp was removed or a biopsy was taken.
The first 24 hours
Most people are told not to drive, drink alcohol, sign important documents, or operate machinery until the next day. Start with foods you tolerate well. Some people jump right back into regular meals. Others prefer bland foods first, such as toast, soup, rice, bananas, eggs, or yogurt.
The next few days
Most patients feel close to normal within a day or two. Mild abdominal discomfort can linger briefly. If you had multiple polyps removed, a large lesion resected, or advanced techniques like EMR, your doctor may recommend temporary diet restrictions, avoiding heavy lifting, or more careful observation for bleeding.
When pathology results arrive
This can take several days to a couple of weeks depending on the lab and the complexity of the tissue. The pathology tells your doctor what type of polyp it was and whether follow-up is needed sooner rather than later.
Possible Risks and Complications
Polypectomy is generally safe, but no medical procedure is risk-free. The most common complications are bleeding and perforation, which means a hole or tear in the colon wall. These complications are uncommon, but the risk can be higher when larger polyps are removed, when electrocautery is used, or when the patient takes blood-thinning medications.
Possible complications include:
Bleeding: Minor bleeding can be normal. Heavy bleeding, persistent bleeding, or delayed bleeding days later needs medical attention.
Perforation: Rare but serious. This may require hospital care or surgery.
Reaction to sedation: Breathing or heart-related reactions can happen, especially in higher-risk patients.
Post-polypectomy coagulation syndrome: This is irritation of the bowel wall after heat-based removal. It can mimic more serious pain but often improves with medical treatment.
Infection or severe abdominal pain: These are less common but should never be ignored.
Call your doctor right away if you have:
Severe abdominal pain, fever, chills, dizziness, weakness, heavy or worsening rectal bleeding, frequent bloody stools, a swollen or hard abdomen, or trouble passing gas. Those are not symptoms to “wait and see” your way through.
What Happens After the Polyp Is Removed?
Once the polyp is removed, the story is not over. The tissue is examined under a microscope to determine the type, size, margins, and any cancerous or precancerous changes. That information helps decide your future screening or surveillance schedule.
In general, follow-up depends on:
How many polyps were found
How large they were
Whether they were adenomas, serrated lesions, hyperplastic polyps, or showed dysplasia
Whether removal was complete and done in one piece or several pieces
Your family history and personal risk factors
For example, a high-quality colonoscopy with no polyps may mean another screening in 10 years. One or two small tubular adenomas may lead to repeat colonoscopy in 7 to 10 years. More numerous, larger, or higher-risk polyps often require a 3-year interval, and piecemeal removal of a large lesion can lead to surveillance as early as 6 months.
Translation: the follow-up timeline is not random. It is built around what the pathology report says and how confident the doctor is that the lesion was completely removed.
Can Polyps Come Back After a Polypectomy?
A completely removed polyp usually does not grow back in the exact same form, but people who have had polyps are more likely to develop new polyps later. That is why surveillance colonoscopy matters. Skipping follow-up is a little like fixing a leak and then deciding you never need to look at the roof again.
You can also reduce future risk by following general colorectal health advice: do not smoke, limit alcohol, stay physically active, maintain a healthy weight, and eat a diet with more fruits, vegetables, and fiber while cutting back on heavily processed and high-red-meat patterns if your doctor recommends it.
What People Commonly Experience After a Polypectomy
Now for the part many medical handouts mention only briefly: the human side. Recovery after a polypectomy is usually medically straightforward, but emotionally and practically, people tend to have a few very common experiences.
First, many people say the prep was the hardest part. Not the procedure. Not the recovery. The prep. The diet changes feel annoying, the laxative drink is rarely anyone’s favorite beverage, and the repeated bathroom trips can make the evening feel much longer than the clock suggests. By the time patients arrive for the procedure, a lot of them are already thinking, “Please let me never romance a sports drink again.”
Second, people are often surprised by how little they remember from the actual procedure. For many, the experience is basically: check in, change clothes, chat with the team, drift off, wake up, wonder what year it is, and then hear someone say the doctor removed a polyp and everything went well.
Third, the first several hours afterward are often described as sleepy and gassy. That is normal. Patients may feel a little bloated, may pass gas more than usual, and may want a quiet couch, a blanket, and a simple meal rather than a heroic return to normal life. Walking around the house can help with the cramping or pressure. Many people feel noticeably better by the evening.
Fourth, there is often a strange gap between “the procedure is over” and “I actually know what they found.” If tissue was sent to pathology, patients can feel fine physically but still anxious mentally while waiting for results. This is common. The waiting period can be more stressful than the recovery itself, especially if a large polyp was removed or if the doctor said the lesion looked unusual.
Fifth, some people are caught off guard by the follow-up conversation. They assume the polyp is gone, so the whole issue is over. But doctors care about more than whether a polyp was removed. They care about the type of polyp, whether it had dysplasia, whether it was removed in one piece, and whether the patient is likely to develop more polyps. This is why one person hears “See you in 10 years,” while another hears “Come back in 6 months.”
Finally, many patients describe a quiet sense of relief afterward. Even if the prep was inconvenient and the waiting was stressful, there is comfort in knowing a suspicious growth is no longer sitting there uninvited. In that way, polypectomy can feel less like a major ordeal and more like smart preventive maintenance. Not glamorous, not fun, but very worthwhile.
Final Thoughts
A polypectomy is one of those medical procedures that can sound scarier than it usually is. In most cases, it is a routine, minimally invasive way to remove a polyp during colonoscopy before it becomes a bigger problem. Recovery is often quick, with most people back to normal activities within a day or two, though larger or more complex removals can require closer follow-up.
The most important thing after a polypectomy is not just healing well. It is understanding your pathology results, knowing your recommended surveillance schedule, and actually following through. Colon polyps are common. So is procrastination. Only one of those should be allowed to stick around.