





Want bakery-pretty sugar cookies without the full-on royal icing marathon? This guide breaks down exactly how to...
An indigo stripe pillow is one of those rare home accents that feels classic, fresh, and incredibly...
Zika virus is quieter than it was during the global outbreak years, but it has not disappeared....
S47 E6: Community Carpenters is more than a recap of a This Old House episode. It is...
Perpeducation blends education and perpetuation to help independent insurance agencies grow future leaders from within. Instead of...
Bundled payments promise better coordination and lower costs, but critics worry they can squeeze quality where patients...

The Halo S3 Pendant is a refined modern glass pendant light designed by David Chipperfield for Wästberg....
Wondering whether a bottle sterilizer is worth the counter space? This in-depth guide explains three practical ways...
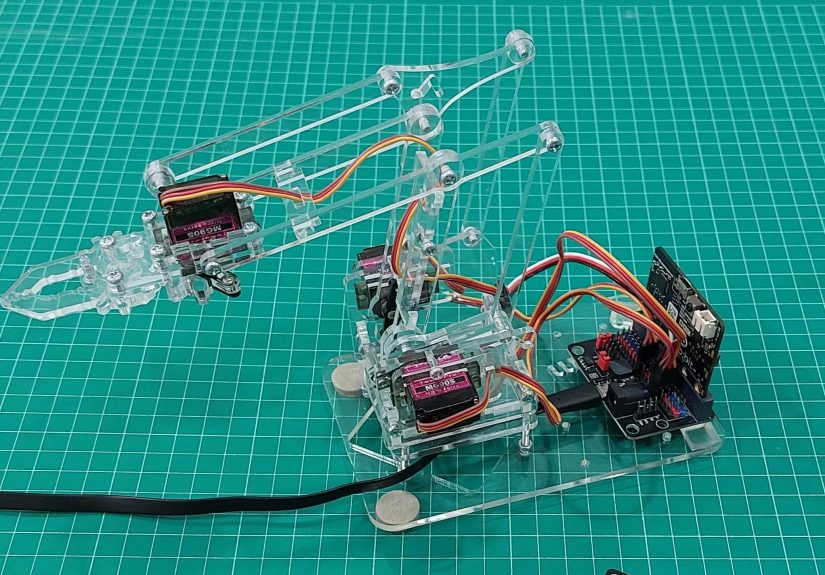
A gesture-controlled robot arm is more than a cool demo. It is a hands-on STEM project that...

Health care success is changing fast. This in-depth guide shows health care professionals how to reinvent their...