
Table of Contents >> Show >> Hide
- First: What “Radiation for Head and Neck Cancer” Usually Means
- Before Treatment: The “Planning Phase” (a.k.a. The Setup That Makes Everything Work)
- During Treatment: What the Daily Routine Looks Like
- Side Effects: The Greatest Hits (and How They Tend to Show Up)
- Nutrition and Hydration: How People Actually Get Through This
- Long-Term or “Late” Effects: What to Watch for After Radiation Ends
- Practical Tips That Make Treatment Feel Less Like a Daily Boss Battle
- After Treatment Ends: The Recovery Timeline (and Why Week 1 Can Feel Like a Plot Twist)
- Real-World Experiences: What Patients Commonly Say It Feels Like (About )
- Conclusion
Radiation for head and neck cancer can feel like signing up for two things at once: a highly precise medical
treatment… and a temporary full-time job where your “office” is a treatment room and your coworker is a
giant machine that does not care about small talk. The good news? Radiation therapy teams do this all day,
every day. They’re pros at guiding you through the weird parts (the mask), the annoying parts (the dry mouth),
and the “why does my throat feel like sandpaper?” parts (mucositis).
This guide walks through what usually happens before, during, and after radiation therapy for head and neck cancers,
plus the side effects people most commonly deal with, how long they tend to last, and what helps in real life.
(Standard disclaimer: your own plan may differ based on tumor location, stage, and whether you’re also getting chemo
or surgery. Always follow your oncology team’s instructions.)
First: What “Radiation for Head and Neck Cancer” Usually Means
For many head and neck cancers, the most common setup is external beam radiation therapyradiation aimed
from a machine outside your body. Treatments are typically given once a day, Monday through Friday, for
about 5 to 7 weeks (often around 7 weeks for many oral cavity/oropharyngeal plans), though schedules can vary.
The “daily” part sounds intense, but each session is usually short; the larger time commitment is getting positioned
perfectly and checking alignment. Some situations use different fractionation schedules, and some plans include chemo
on the same day.
Common radiation types you may hear about
- IMRT (Intensity-Modulated Radiation Therapy): A highly shaped approach that helps focus dose on the tumor and reduce dose to normal tissues when possible (like salivary glands).
- IGRT (Image-Guided Radiation Therapy): Uses imaging during treatment to improve accuracy and day-to-day consistency.
- Proton therapy (in select cases): Uses protons instead of X-rays; for some head/neck tumors, it may reduce dose to nearby healthy tissues depending on anatomy and plan design.
Before Treatment: The “Planning Phase” (a.k.a. The Setup That Makes Everything Work)
1) Consultation and team check-ins
Expect a visit with a radiation oncologist (the doctor who directs your radiation plan) and often a wider team:
nurses, radiation therapists, dietitians, dentists, and sometimes speech-language pathologists (SLPs) who help protect
swallowing and speech.
2) Dental evaluation (seriously, don’t skip this)
Radiation to the head and neck can reduce saliva and increase risk of dental problems (including cavities), and can make
future dental extractions riskier for the jaw bone. Many patients are advised to get a dental exam and address high-risk
issues before treatment starts. You may also hear about fluoride or special dental care routines to reduce long-term tooth
damage.
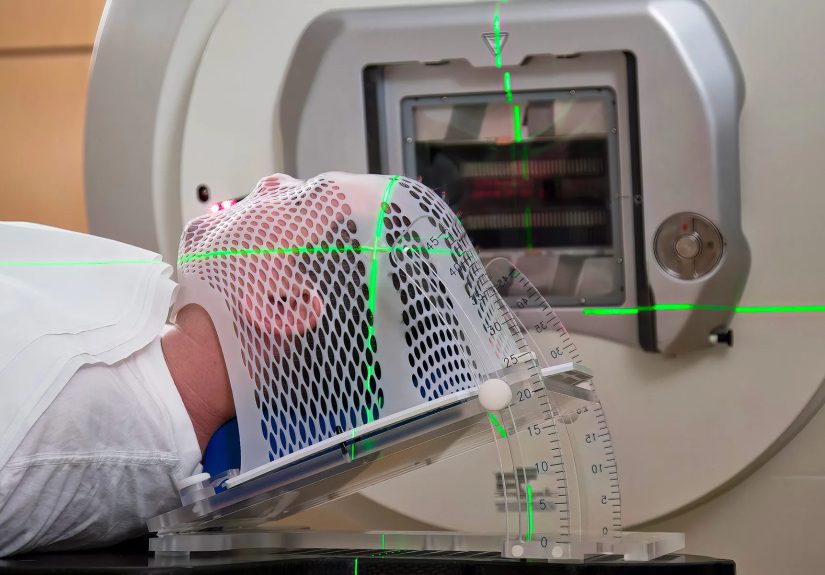
3) CT simulation and the immobilization mask
This is the appointment where your team maps out your treatment. You’ll typically get a CT scan in the exact position
you’ll be treated in. To help you stay perfectly still and consistent, many head and neck patients get a custom
thermoplastic mask over the head/neck/shoulders. It’s molded to you while warm, then hardens. It can feel
a little “space-helmet chic,” but it’s one of the reasons radiation can be delivered so accurately.
Pro tip: if you’re worried about claustrophobia, tell your team before mask-making day. They can coach breathing
techniques, music options, and (in some cases) medication strategies. Nobody wins awards for suffering silently.
4) Skin marks and positioning
Many centers use small marks (sometimes tiny tattoos or semi-permanent ink) to help line you up the same way each day.
This isn’t body art; it’s GPS for your treatment plan.
During Treatment: What the Daily Routine Looks Like
Your schedule
Most people come in every weekday for several weeks. Some centers schedule a weekly “check-in” visit during
treatment to monitor side effects, weight, hydration, pain control, and skin/oral changes.
What happens in the room
- You’ll lie on the table, get positioned, and the mask is secured if you have one.
- Therapists step out while the machine delivers radiation. You’re monitored the entire time.
- The machine may rotate around you; it does not touch you.
- Radiation itself doesn’t hurt during delivery. The side effects build over time.
Side Effects: The Greatest Hits (and How They Tend to Show Up)
Most head and neck radiation side effects are related to irritation and inflammation in tissues that are sensitive
(mouth, throat, skin) and to reduced function in glands and muscles involved in saliva and swallowing. Side effects
commonly start gradually, build week by week, and often peak near the end of treatment and the couple of
weeks afterward. Then, recovery beginsslowly, but it does begin.
Mouth and throat soreness (mucositis) + swallowing difficulty (dysphagia)
Mouth and throat soreness can range from “spicy salsa regrets” to “I would like to file a formal complaint against soup.”
Inflammation and ulcers can make eating painful. Swallowing may become harder as tissues get irritated and as muscles
weaken or stiffen over time.
Many teams recommend a consistent mouth-care routine (often salt/baking soda rinses, depending on your center’s protocol),
pain control plans, and early involvement of speech/swallow therapy. Doing swallowing exercises during treatment can help
preserve function and reduce long-term problems.
Dry mouth (xerostomia) and thick, sticky saliva
Radiation can affect salivary glands, leading to reduced saliva (dry mouth) and sometimes thick, stringy secretions that
feel like your body accidentally ordered “industrial-strength glue” instead of saliva.
A common pattern is: saliva decreases early, then secretions can become thick and sticky by weeks 3–4,
and may stay that way through treatment. Dry mouth can also raise the risk of dental issues and oral infections, which is
why dental prevention and meticulous oral hygiene matter so much.
Taste changes and appetite drop
Taste can change dramaticallyfoods may taste bland, metallic, or “off.” Smell changes can add to it. This often contributes
to weight loss risk because eating becomes less enjoyable and more work. Nutrition is not a side quest here; it’s part of
treatment.
Skin changes on the neck/face (like a sunburn, but stubborn)
Skin in the radiation field can redden, darken, itch, peel, or become tenderoften starting a couple of weeks in and
worsening over time. Your team will have skin-care recommendations (usually gentle cleansing, avoiding irritants, and using
approved moisturizers). Don’t freestyle new creams without checking; some products aren’t recommended during treatment.
Fatigue
Fatigue from radiation is common and can build across weeks. It’s not always “sleepy tired”it can feel like your body is
running on low battery even after rest. Planning for lighter schedules, accepting help, and prioritizing nutrition/hydration
often makes a real difference.
Voice changes, hoarseness, and cough
If the radiation field includes the larynx or nearby tissues, hoarseness and throat irritation can happen. Some people also
notice cough or phlegm changes.
Nutrition and Hydration: How People Actually Get Through This
What “eat what you can” really means
Many patients do best with soft, moist foods that are easier to swallow (think: scrambled eggs, smoothies,
oatmeal, soups, yogurt). Spicy, acidic, and rough foods (chips, crusty bread) can be brutal when mucositis hits.
Your team may suggest high-calorie shakes or oral nutrition supplements when appetite drops.
Feeding tubes: sometimes needed, sometimes not
Not everyone needs a feeding tube. Many people can continue eating by mouth (with modifications) throughout treatment,
and many centers emphasize swallowing therapy and symptom management to help avoid tube dependence. But if swallowing is
unsafe (aspiration risk) or you can’t maintain weight/hydration, a temporary feeding tube may be recommended. Even with a
feeding tube, patients are often encouraged to keep swallowing safely if possible to preserve function.
Long-Term or “Late” Effects: What to Watch for After Radiation Ends
Many side effects improve in the weeks to months after treatment. Some can linger, and a smaller portion can become
long-term issuesespecially in higher-dose areas or when combined with chemotherapy or surgery. Your team will monitor you
and help manage late effects.
Dry mouth and dental risk
Dry mouth can persist and may increase risk of cavities, gum disease, and oral infections. Ongoing dental care, fluoride
strategies, and regular checkups are commonly recommended.
Jaw stiffness (trismus) and tissue tightness (fibrosis)
Radiation can cause scarring and tightening over time, which may reduce mouth opening or create stiffness in the jaw/neck.
Jaw stretching and therapy exercises may be recommendedstarting early can help.
Thyroid changes
When the thyroid is in or near the radiation field, thyroid function can decrease over time. This is often monitored with
blood tests after treatment, because hypothyroidism is treatable but easy to miss if you assume fatigue is “just life now.”
Bone and soft tissue effects (including osteoradionecrosis)
Rare but important: radiation can affect jaw bone healing capacity, which is why dental planning matters and why your dentist
should know your radiation history before extractions or major procedures.
Practical Tips That Make Treatment Feel Less Like a Daily Boss Battle
- Start mouth care early: Don’t wait for soreness to begin. Consistent rinses and hygiene can help reduce complications.
- Track weight weekly: Small drops can snowball fast when eating hurts.
- Hydrate like it’s your job: Dry mouth + thick secretions are easier to handle when you’re well-hydrated.
- Do the swallowing exercises: They can feel silly. Do them anyway. Your future self may send a thank-you card.
- Tell your team about pain early: There are stepwise optionstopical rinses, meds, nutrition adjustments, and more.
- Bring a “treatment bag”: Water, lip balm, tissues, lozenges (if approved), and a small snack for after.
- Ask what’s normal vs. urgent: Fever, inability to swallow fluids, uncontrolled pain, dehydration signs, or breathing trouble should be addressed promptly.
After Treatment Ends: The Recovery Timeline (and Why Week 1 Can Feel Like a Plot Twist)
A common surprise: some side effects can feel worse for a short time after the last radiation session. That’s
because inflammation doesn’t instantly shut off when the schedule ends. Many people start to turn the corner in the weeks
that follow, with gradual improvements in swallowing comfort, skin healing, and energy. Taste and dry mouth can take longer,
sometimes months, and occasionally longer-term management is needed.
Follow-up visits matter. Your team checks healing, nutrition, swallowing, and monitors for late effects like thyroid changes.
Bring a list of symptoms (even the weird ones). The “electric shock feeling when bending your neck” type of symptom exists
in medical literatureif something feels odd, you’re not being dramatic.
Real-World Experiences: What Patients Commonly Say It Feels Like (About )
People often describe head and neck radiation as a marathon made of tiny daily sprints. The first week can feel deceptively
normallike, “Wait… that’s it?” The sessions are quick, nothing hurts during treatment, and you might leave thinking the
internet was being a little dramatic. Then week two arrives with a reminder that your body did, in fact, notice the radiation.
Dry mouth often shows up early: you wake up feeling like your tongue spent the night camping without a water bottle.
Around weeks three and four, many patients report that the mouth/throat irritation becomes the main character. Eating shifts
from “I’m hungry” to “What foods can I tolerate without regretting my choices?” This is when soft, moist foods become best
friends, and nutrition shakes stop being an occasional convenience and become a strategy. Some people joke that they develop
a refined palate for which brand of shake is “least offensive,” which is both funny and… extremely practical.
The mask experience varies. Some people say they adapt quickly and it becomes routine: lie down, click, breathe, done.
Others find the first few sessions claustrophobic and need a game planmusic, guided breathing, counting backward, or asking
the team to talk them through the first minute. A common theme: telling the team early helps a lot. Radiation therapists have
seen every version of “I’m fine” that is actually “I am not fine,” and they’re usually great at helping you feel in control.
The “thick saliva” stage gets described in creative ways“sticky,” “stringy,” “like glue,” “like my mouth is producing its
own special effects budget.” People carry tissues, sip water constantly, and rinse frequently. Nighttime can be tough when
secretions build up, so sleeping with your head slightly elevated and keeping water nearby is a common workaround (ask your
team what they recommend).
Fatigue is another frequent surprise. It’s not always the kind that improves with a nap. Many describe it as a full-body
heaviness that builds slowly. The most helpful mindset tends to be: treat fatigue like a real symptom, not a personal failing.
Short walks can help some people, but rest and pacing are key. On the emotional side, patients often say it helps to measure
progress in small wins: finishing the week, maintaining weight, getting through a rough patch without missing sessions, or
finding one meal that still tastes okay.
Finally, many people say the end of treatment is both a relief and a curveball, because side effects can peak right after the
last session. Knowing that can prevent panic. Recovery is typically gradualmore “slow fade” than “instant reset.” Patients
who feel best supported often lean on the whole care team: oncology, nursing, dental, nutrition, and speech/swallow therapy.
And yespeople really do get back to enjoying food again. It just might take time and some very patient taste buds.
Conclusion
Radiation therapy for head and neck cancers is intensely targetedand it can also be intensely inconvenient. Expect a planning
phase (consults, dental prep, CT simulation, mask), a daily weekday treatment routine for several weeks, and side effects that
usually build over time: mouth/throat soreness, dry mouth, thick saliva, taste changes, skin irritation, fatigue, and swallowing
challenges. The best outcomes aren’t just about the radiation planthey’re also about the support plan: oral care, nutrition,
hydration, pain management, and swallowing exercises. Bring your questions, report symptoms early, and let your team help.
That’s what they’re there for.






