



A tiny simple white bell may look modest, but it carries surprising design power. This in-depth article...
Walmart’s Cyber Monday generator deals can be genuinely worth the hype, especially if you know the difference...
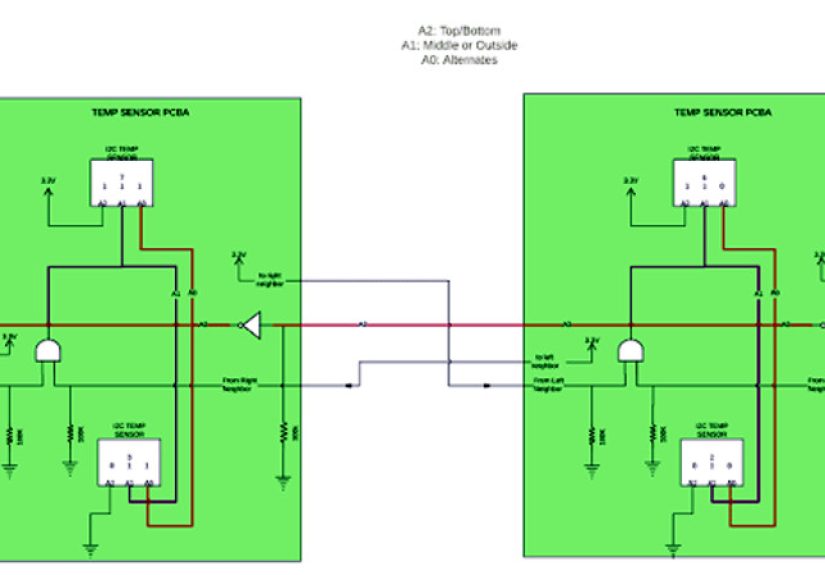
Automatic I2C address allocation sounds like plug-and-play magic, but real success comes from smart system design. This...
What happens when regular coffee drinkers switch to alternatives like green tea, matcha, chicory, herbal tea, decaf,...
Target Cyber Monday is where budget decor meets surprisingly good furniture and practical home upgrades. This in-depth...

Picking paint gets much easier when you know how to use color swatches the right way. This...

Want a door that closes smoothly instead of slamming like it is auditioning for a soap opera?...
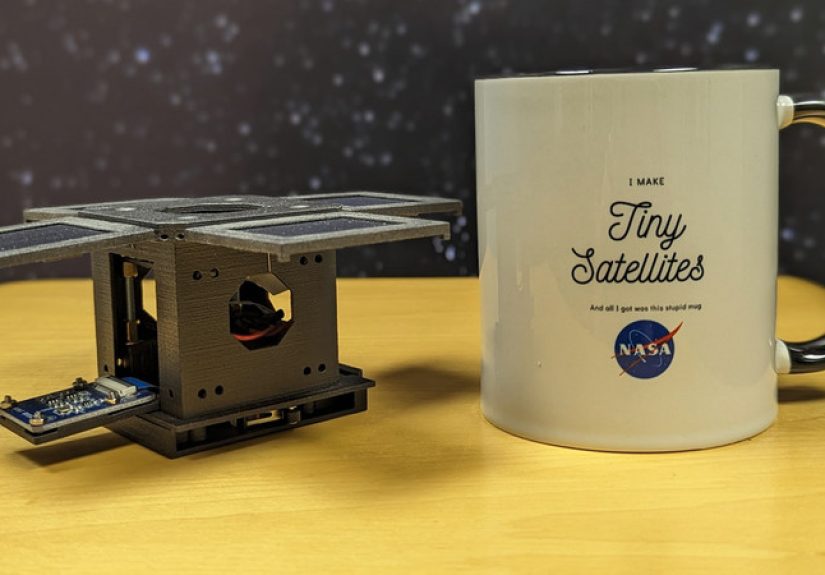
Space is no longer just for giant agencies and giant budgets. This in-depth article explores how picosatellites,...
Can an Accurate Omegaverse Quiz really deliver a 100% guarantee? Not literally, but the best ones can...

Essential fatty acids (EFAs) are the fats your body can’t make but absolutely needsmainly linoleic acid (omega-6)...