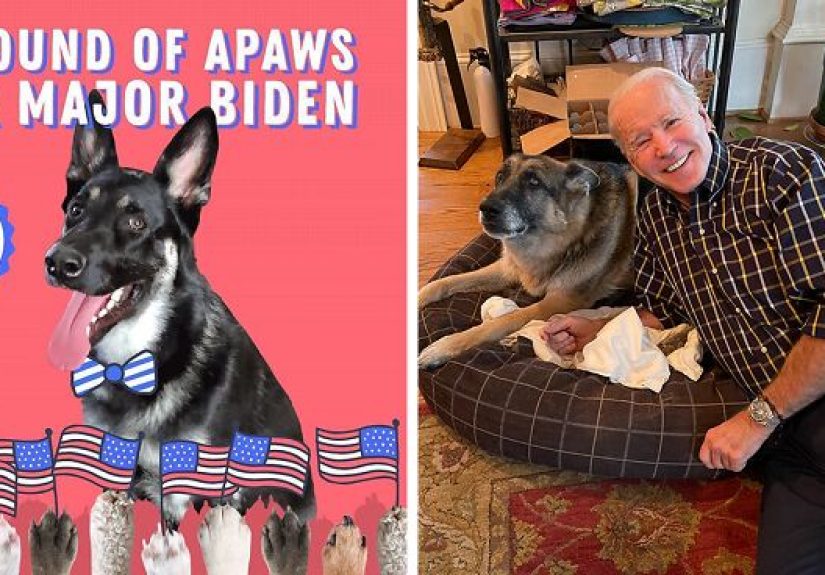




Major Biden’s virtual “indoguration” was more than a cute internet event. It celebrated the first shelter dog...
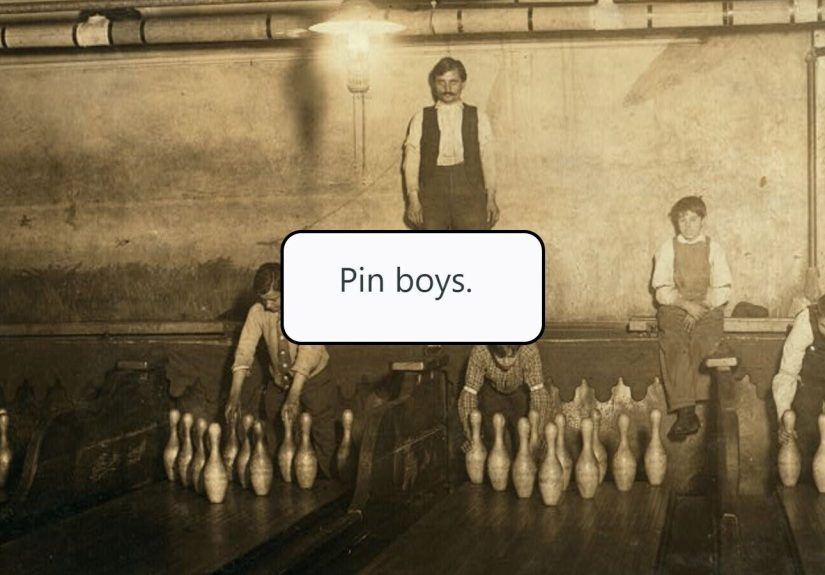
From lamplighters and icemen to switchboard operators and video store clerks, many once-essential jobs have disappeared as...
Need more storage for your Wii U? This guide explains five practical ways to set up an...
College can look exciting from the outside, yet many students are quietly battling anxiety, burnout, loneliness, and...
Energy drinks can deliver a quick boost, but the trade-off is often high caffeine, added sugar, sleep...

Want to learn how to do the country two step without feeling like your boots are freelancing?...

Mercury glass globe string lights blend vintage sparkle with modern versatility, making them a favorite for patios,...
Suspect he’s lying but do not want to sound dramatic? This guide explains how to tell a...

What does it really feel like to step inside the home of a Dutch artist? This in-depth...

Commune’s black-and-white concrete tiles are more than a surface choicethey are a design statement with staying power....